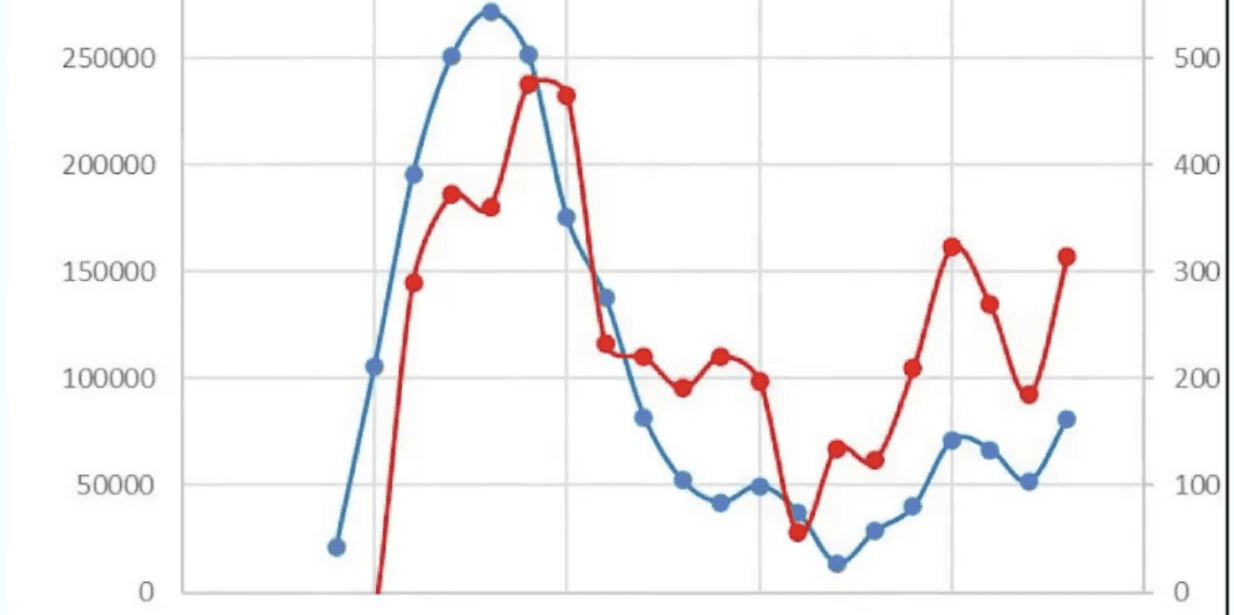
The elites are ignoring massive death numbers. Data doesn’t lie. Dr. Theo Schetter, a vaccinologist based in the Netherlands who has played a leading role in the development of a number of vaccines, has analysed the official data from the Dutch Government and found a very close correlation between when fourth vaccine doses were administered in the country and the number of excess deaths, as shown in the chart below. Importantly, in the Netherlands the booster rollout in different regions was staggered over a number of weeks allowing an analysis by region, which confirms the effect.
Data doesn’t lie: mRNA-vaccines and correlation to all-cause mortality
Marlies Dekkers speaks with with Drs. Robert Malone and Theo Schetters
Dr. Schetters, a recipient of the Medal of Honour of the Faculty of Pharmacy at the University of Montpellier in France, told Dr. Robert Malone that doctors are currently seeing “all sorts of symptoms that they do not know what it is” and that “in the Netherlands now it’s very clear that there is a good correlation between the number of vaccinations that are given to people and the number of people that die within a week after that.” It is essential to look at all-cause mortality, he said, as the vaccine “potentially affects all organs.”
“…So it potentially affects all organs. And that’s what the medical doctors now see, they see all sorts of symptoms that they do not know what it is. And because the adverse effects are so not just single one adverse effect, but can be anything, they surface very difficult to a statistical level. And that’s why we do analysis on all-cause mortality, because say, okay, and if we do not know what is exactly related to vaccination, of course, the coagulation problems, myocarditis, we know that, but there are many more things happening at the moment. And so that’s why we look at all-cause mortality, and in the Netherlands now it’s very clear that there is a good correlation between the number of vaccinations that are given to people and the number of people that die within a week after that. So let’s say in this week we gave 10,000 vaccinations. Then in this week, we have something like 125 excess in death in that week.”
The correlation is striking, he said, to the extent that if you have more vaccines in a week then you also have more excess deaths, and if you have fewer vaccines in a week, you have fewer deaths. Dr. Schetters says he has written to the Director of the Institute of Health in the Netherlands to alert him to the findings.
“…So what we’ve done is we have written a registered letter to the director of our Institute of Health and presenting the results and expressing my concerns. And just with the question, from a precautionary point of view, please reconsider vaccination strategy because I think this is a real warning. And so it’s not that everybody dies. Actually I do a rough calculation, it’s one in 800.”
During the interview, Dr. Malone explained that his own organisation, consisting of 17,000 medical practitioners and scientists, has released a statement that the vaccines should be withdrawn as they are no longer justified on a risk-benefit ratio, a statement with which Dr. Schetters agreed.
Dr. Malone said:
“I stand as the President of the International Association of Physicians and Medical Scientists. So we’re 17,000 that are only physicians and medical scientists, all verified, no nurses, not because we don’t like nurses, but it has to do with the positioning with the press and messaging. So that’s the basis for our organisation. “Months ago, we came out with a press conference in a clear unequivocal statement that one can find at www.globalcovidsummit.org where we made a clear, unambiguous statement. In our opinion, as an organisation, these vaccines should be withdrawn. They are no longer justified on a risk-benefit ratio. And as the person who is responsible for the genesis of this technology, I’m often criticised. Didn’t I realise what I was doing? And there’s no way for me to have known that the normal standards for regulatory development and testing and clinical would be circumvented. “But I stand as someone who has intimate, detailed knowledge of the technology and its risks and benefits, the nature of the formulations, the role of the pseudouridine, [Pseudouridine is the most abundant modified type of nucleoside across all species of RNA] all of those things. It’s my opinion and that of the organisation that I represent, that the data are now sufficiently clear that, in our opinion, the ongoing campaign for vaccination is no longer warranted.”
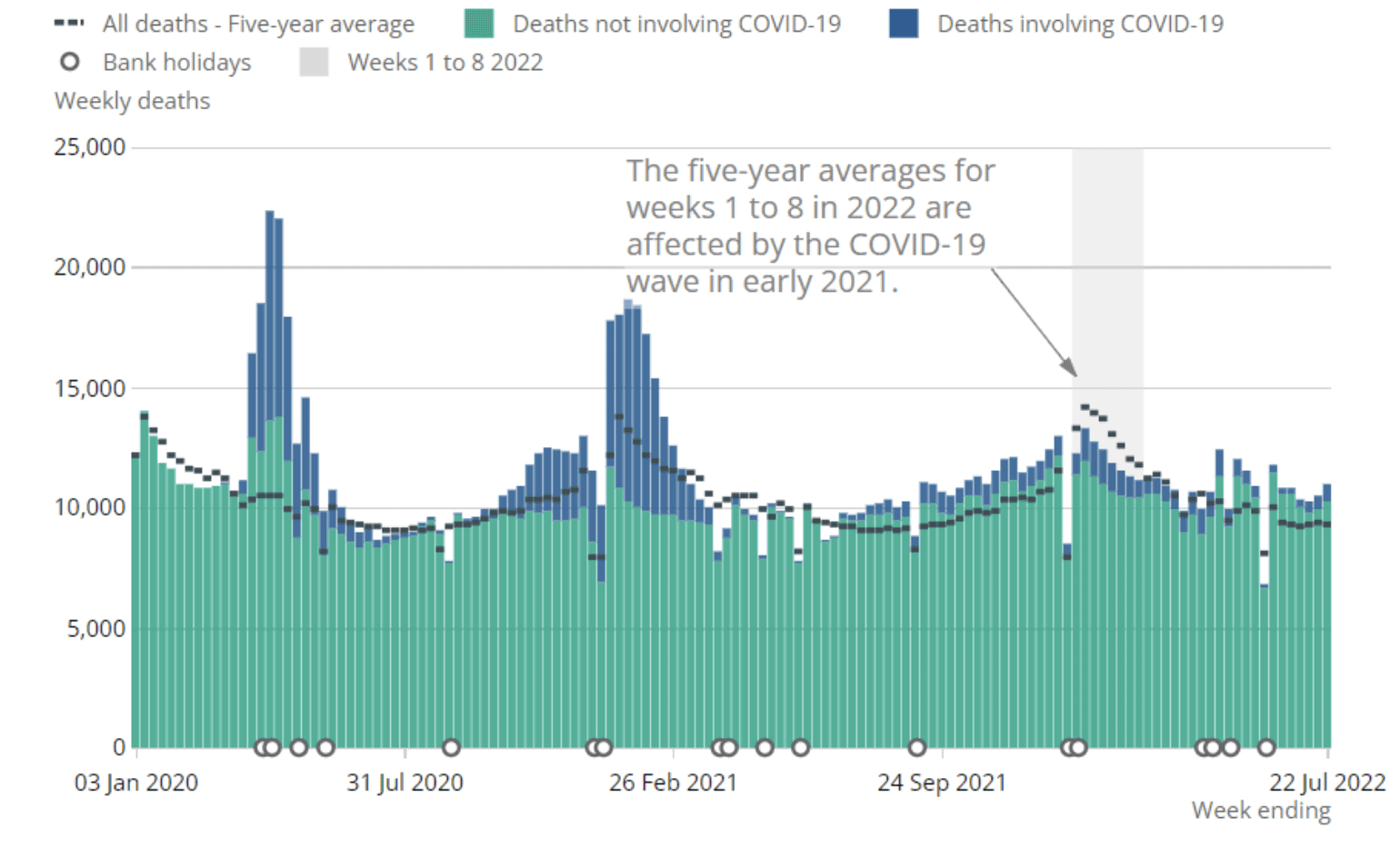
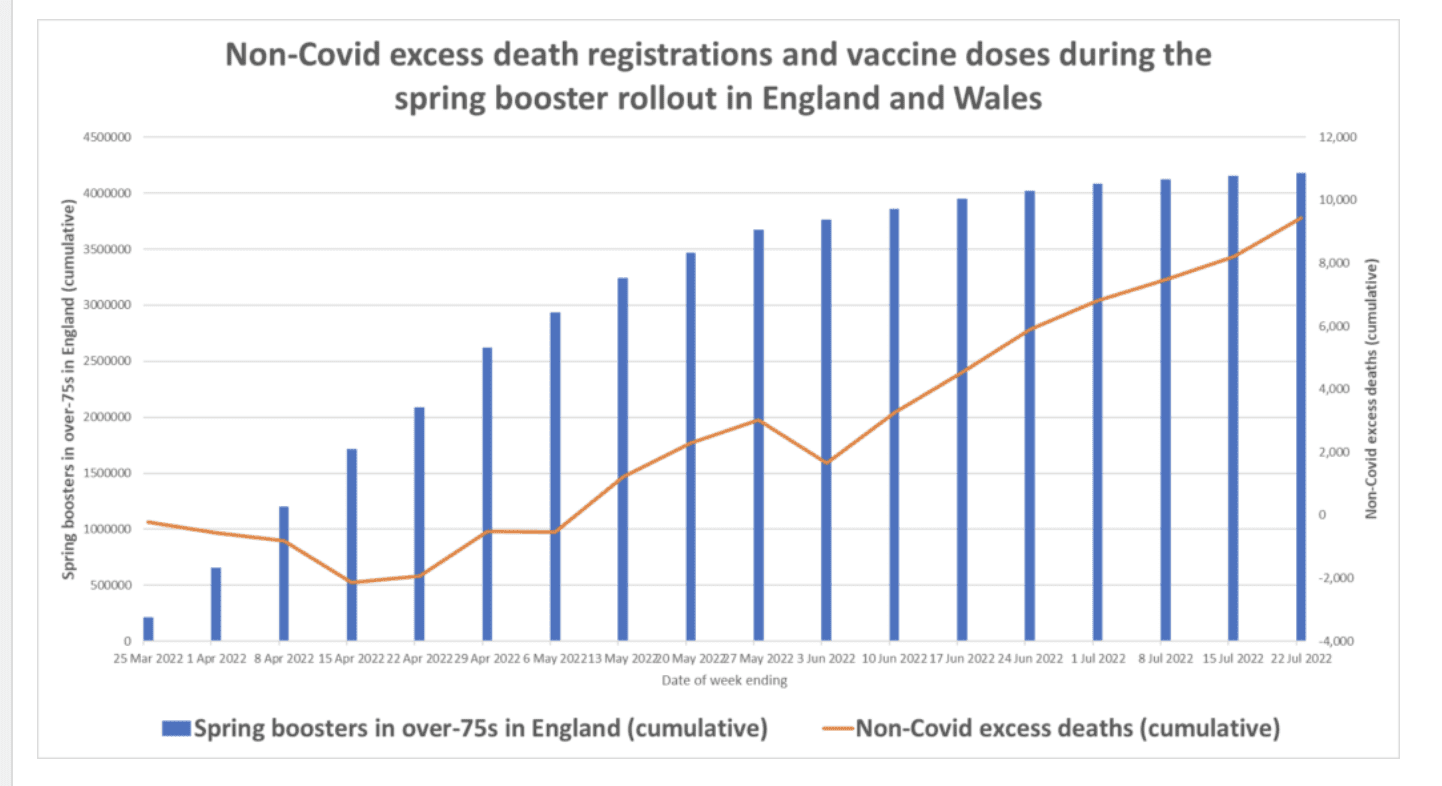
Dr. Schetters’ analysis is in line with the observations other experts have been making as they have followed what appears to be a correlation between the spring fourth dose booster rollout among over-75s in England and a wave of now over 11,000 non-Covid excess deaths that are currently unexplained (see the charts below).
The latest official data from the Office for National Statistics from August 2nd shows there has been 11,370 excess non-Covid deaths registered in England and Wales in the 13 weeks since April 23rd. If all of these were a result of the spring boosters (of which 4,182,483 have been delivered up to July 22nd) it would be a rate of one every 368 doses. That figure is an upper bound, as not all the additional deaths will be due to the boosters, but it shows the British data are broadly in line with the Netherlands data. Note that a higher vaccine injury rate would be expected in Britain where the fourth doses are only being given to the over-75s, as the rate increases with age.
In the week ending July 22nd, 10,978 deaths were registered in England and Wales, which is 1,680 (18.1%) above the five-year average for the week. Of these, 745 mentioned COVID-19 on the death certificate as a contributory cause and 463 mentioned COVID-19 as underlying cause, leaving 1,217 deaths from a different underlying cause. Note that this was the week of the brief but intense heatwave (with recorded temperatures topping 40°C for the first time in some areas), so some of these will be heatwave deaths, as will many of the additional Covid deaths (being people who happened to have Covid at the time).
Deaths by date of occurrence rose dramatically in the most recent week, which might be assumed to be connected with the heatwave of July 18-19th, but the data by date of occurrence show the spike occurring in the week ending July 15th, too soon for the heatwave. One explanation for this may be that the ONS uses a ‘statistical model’ to calculate death occurrences for recent weeks and this model may not cope well with unpredictable phenomena like heatwaves. If so, we should see adjustments in the next few reports as more real data become available. Note that the cause of the spike in non-Covid excess deaths during June remains unclear.
Here is the cumulative curve of excess non-Covid deaths by date of registration along with the cumulative total of spring boosters.
As noted in previous weeks, the cause of the deaths appears to be largely related to diseases of the heart and blood vessels (cause of death data for July are now available here https://tinyurl.com/y629d2tv ). Cancer deaths are broadly at normal levels, suggesting there is something other than lack of access to healthcare going on. The continued high level of excess deaths is unexpected as, following the 142,000 excess deaths of the last two and a half years, we would have anticipated a period of lower than average deaths.
The British Government has shown no interest in investigating what lies behind the more than 11,000 additional deaths in three months. When Member of Parliament Esther McVey, Chair of the Pandemic Response and Recovery All-Party Parliamentary Group (APPG), submitted a written question asking the Cabinet Office what steps it was taking “to investigate the higher than expected rate of deaths of 12.2% above the five-year average” it fobbed her off with the reply that referred her to the U.K. Statistics Authority, which, in turn, fobbed her off with the reply that merely said it will continue to publish the relevant statistics.
Background: Dr. Theo Schetters obtained a PhD in Medicine from Nijmegen University in the Netherlands, and received a visiting scientist award from the Royal Society (London) to work on malaria immunology at the National Institute for Medical Research in Mill Hill, London (UK). From 1988 to 2014 he worked at Intervet International (Boxmeer, The Netherlands) where he developed a vaccine against coccidiosis in chickens (Nobilis® Cox ATM) and a vaccine against Babesia infections in dogs (Nobivac® Piro). He is inventor of an improved vaccine formulation against diseases associated with Rhipicephalus ticks. Presently, he is director of ProtActivity, a company that focuses on vaccine development against ticks and tick-borne protozoal infections. In 2004 he received the Medal of Honour of the Faculty of Pharmacy, University of Montpellier 1 in France and was bestowed Professeur Invité as recognition for his contribution to longstanding collaborative research with the Laboratory of Cellular and Molecular Biology of the University (head Prof. Andre Gorenflot). He is an editorial board member of “Veterinary Parasitology, Trials in Vaccinology” (Elseviers Science Publishers) and “Parasitology” (Cambridge University Press).
Dr. Schetters is an exceptional, gifted, and highly respected vaccinologist – let us hope his warnings will not be ignored by his government and world health leaders.
This is a long interview. Therefore, I have edited the transcript below to focus on his latest study, which statistically tests the possibility of correlation of the booster vaccine campaigns (in the 60+ year cohort) in the Netherlands to excess all-cause mortality. The hypothesis basically being that there is a temporal (time) statistical correlation between regional vaccine uptake and spikes in excess all cause mortality in the 60+ cohort of vaccine recipients. The government of the Netherlands has employed a strategy of deploying “booster” doses of the genetic vaccines as regional vaccination waves, which provides an opportunity to examine possible correlations after sorting data by time and region. This enables a form of internal controls in the data analysis approach, which can be used to increase the power of the analysis. Theo has now sent that data to the Government of Holland. I think his study may be one of the most important to become available this year, because the correlation linking the vaccines and excess mortality in the tested (60+ year) cohorts appears to be extremely strong.
I look forward to these results being submitted, peer reviewed and published in a peer reviewed journal, although I am wary that the political implications of his findings may make it difficult to find a journal editor willing to stand up to the likely political backlash. In the video and the transcripts, Theo provides a taste of the data that he is now sitting on. If these data and analyses withstand further scrutiny, as I think they will, the findings will either force policy changes or will further validate the compromise of the independence and integrity of global public health policymaking processes and decision makers.
Excepts from Transcript (because of accent/second language issues, the transcript is not 100% perfect, please forgive any blips with sentence structure and grammar) –
Dr. Theo Schetters: The thing that we knew from the beginning, was that COVID (SARS-CoV-2) was a very mutating virus. So I always said, it’s like you run with your syringe behind the virus, that’s running away from you. And so you can never keep up with the mutations. And that is actually that’s what we see now.
So also the Netherlands, the National Institute of Health has said that people that have been vaccinated twice with the original vaccine, that at this moment there is zero protection anymore. So that’s official result, that on the efficacy side (zero protection).
Then on the safety side, we also see problems. That’s the most difficult part because people (the government) do not want to talk about the safety. There’s so many people that contact me because in the Netherlands, I’m some sort of famous. So I get emails and phone calls of people who have had very bad experiences after vaccination.
And the sad thing is that, although these people obeyed the rules of the government and trusted them, now that they have these terrible side effects, the government doesn’t want to listen. You know, they are just so neglected. We don’t talk about it. And that’s the situation at the moment.
I sometimes make the comparison that there was a murder and then the body was thrown into the lake. And after a certain time that body surfaces, and this is what we see happening now, and that’s a very difficult, very difficult story.
These vaccines are here on the market. These companies earn an awful lot of money. Why aren’t these companies not doing the research that we ask for? Because now, if we talk about is there any risk that you get changing your DNA because of this technology, that research is being done by academics, by research groups who do it on Friday afternoons, because nobody wants them to do it (they are not paid to do it). And that’s what now happens. When will all these companies have the money and the means and everything to do that?
Dr. Robert Malone: … I’ve seen it all. The rule in drug development is that if you’re in the pharmaceutical industry, you never ask any question that you aren’t forced to ask because you may get an answer that you don’t like.
Dr. Theo Schetters: Exactly, yeah.
Dr. Robert Malone: And this is explicit. The reason why the pharmaceutical companies are not doing it is it’s not in their financial interest to do so. And the regulators have failed in requiring, in doing their job, in requiring that FDA, EMA, fill in the blank. Okay? The global regulatory community has failed to do its job of insisting on the correct application of the guidance in the international committee on harmonization and the EMA and FDA regs to insist that the pharmaceutical industry does its job. That’s how that’s ecosystem works. Pharma will not do those studies. And governments will not fund those studies unless there is a forcing function that says you will do those studies because we have all agreed, and we have, all of the regulations and documentation say that these things should have been done.
Dr. Theo Schetters: Yeah, exactly.
Dr. Robert Malone: There was a conscious decision to not force the pharmaceutical companies to do the things that the regulations require, that we’ve all agreed upon over decades…
Dr. Theo Schetters: Just thrown away.
Dr. Theo Schetters: So how are we going to bring this message to the public? Most of the people are vaccinated in the Netherlands. It’s something like 75%. So you cannot freak them out by saying you have something in your body that’s going to be the end of your life. No, because that’s what I’m trying to say. In all fairness, it (the probability of death attributable to vaccine acceptance) isn’t that strong.
We know that it’s not like that everybody is dying within a year after you’ve been vaccinated, but a certain percentage of the people have big problems with this. And the point is that I think we have to be open and fair about this. Not only because of the Corona vaccines, but because what we see happening is that this technology is being sort of introduced as, now we’ve used it in Corona, it’s accepted. Everybody knows that. mRNA vaccines, you know?
Dr. Robert Malone: Influenza. Monkeypox (mRNA vaccines are coming)
Dr. Theo Schetters: Exactly. So, and that’s what we are fighting against, because we say this technology is not mature and maybe it can do something in the future, but we are certainly not at the point now to develop all these other vaccines or variants, like an Omicron variant Corona vaccine with the same technology known, because you didn’t solve that problem. And we have that problem. We have a problem of people dying after vaccination. And getting sick.
Dr. Robert Malo…: Including the children.
Dr. Theo Schetters: Yeah.
Dr. Robert Malone: And having reproductive health consequences.
Dr. Theo Schetters: Yes.
Marlies Dekkers: So what do we now know then about the side effects? So this is the future. Sounds horrible to me. But in the now, what can people be aware of? What kind of complaints that they can have or what kind of that they now listen to this and think ‘what?’, it’s connected perhaps to the vaccine.
Dr. Theo Schetters: Yeah. Well, and that’s the problem with this technology because this mRNA travels through your body because of the formulations that they used.
Dr. Robert Malo…: Which physicians were told was not the case.
Marlies Dekkers: No, it should stay in the arm.
Dr. Theo Schetters: So it potentially affects all organs. And that’s what the medical doctors now see, they see all sorts of symptoms that they do not know what it is. And because the adverse effects are so not just single one adverse effect, but can be anything, they surface very difficult to a statistical level. And that’s why we do analysis on all cause mortality, because say, okay, and if we do not know what is exactly related to vaccination, of course, the coagulation problems, myocarditis, we know that, but there are many more things happening at the moment. And so that’s why we look at all cause mortality, and in the Netherlands now it’s very clear that there is a good correlation between the number of vaccinations that are given to people and the number of people that die within a week after that. So let’s say in this week we gave 10,000 vaccinations. Then in this week, we have something like 125 excess in death in that week (My note – that equals 800 deaths per 100,000 or 1/800 in the 60+ cohort).
Marlies Dekkers: And what kind of data then you use?
Dr. Theo Schetters: I use the data from the Central Bureau of Statistics and of our National Institute of Health. And the point is that although they report that every week, they do not report the graphs that we make. So what they do is they show the cumulative buildup of the people, the number of people that have received the vaccination, the fourth injection. So then you see a curve that goes up. You do not see the change per week, but if you calculate a change per week and you then take the figures from the Central Bureau of Statistics, where they present you the excess mortality that follows the same dynamics, the same.
Marlies Dekkers: So if you have more vaccines in that week, then you also have more excess death.
Dr. Theo Schetters: Exactly. Yes.
Marlies Dekkers: If you have less vaccines in that week, you have less…
Dr. Theo Schetters: Fewer deaths.
Marlies Dekkers: I got goosebumps.
Dr. Theo Schetters: Yeah. And the point is, of course, we do not get the real, what we call the granular data, which means that we do not have this from person by person. These are group type figures. So that group received that number of vaccines. And in that age group, you see this number of excess mortality. But we do not know whether this is really correlated one by one. And so that’s why we asked for more data, because Ronald Meester said – Ronald Meester is a professor in statistics and we’ve discussed it here and said, okay, give us those data within a week.
We know what’s happening. Simple. But we can’t get the (granular) data. So that leaves us with a correlation, with an observation. But I think, by now, it’s getting so strong that at least, if you talk about precautionary measures- that’s the way they sold the vaccines, actually, they sold them as precautionary measures. So to keep us safe. Then I would say, I use the same argument now. If I see these correlations, although I cannot prove causality at the moment, from a precautionary measure, you should say let’s stop this.
Dr. Robert Malone: So all-cause mortality is the ultimate indicator for things that we didn’t expect. And that’s why we always have to have it in clinical research. And yet once again, like so many other things, we have disregarded the learning of decades and denied the importance of all-cause mortality.
Dr. Theo Schetters: Yeah. So what we’ve done is we have written a registered letter to the director of our Institute of Health and presenting the results and expressing my concerns. And just with the question, from a precautionary point of view, please reconsider vaccination strategy because I think this is a real warning. And so it’s not that everybody dies. Actually I do a rough calculation it’s 1 in 800, but then again, but I mean, these are then especially…
Dr. Robert Malone: 1 in 800 is a pretty big number.
Marlies Dekkers: It’s a pretty big number.
Dr. Robert Malone: The myocarditis incidence now is publicly acknowledged by some governments as 1 in 5,000.
Dr. Theo Schetters: Yeah, I know. And so when I talk about, of course, the (booster) vaccination campaign that’s now going on, that’s the nice thing in the Netherlands it’s done in campaign. So if you have a danger signal that comes easier to the surface…with a … time window, so you can easily…
Marlies Dekkers: …follow it up.
Dr. Theo Schetters: (The booster) That’s given only to people of 60 plus age. Yeah? So that maybe explains why you have a relatively high number, because you also have the very old who are (dying in higher numbers from the vaccine).
Dr. Robert Malone: So this is crucial, and this was something that was pulled out of the early data at least a year ago is, and it was one of the logic flaws that I had made and others had made, we criticized the CDC and these other public entities for not stratifying the risk of the virus, meaning the truth is that virtually all of the risk for death of the virus is isolated in a very small age window of really 65 and above.
I wrote op-eds with Peter Navarro saying we should focus our vaccination just on these people that need it most and let the rest of the population be more like what Sweden eventually did, and acquire natural immunity and save the vaccine rather than driving the evolution of vaccine escape mutants for these people that needed it most.
And then the data came out that not only is the risk of the virus stratified by age, but the risk of the vaccine is stratified by age.And when you do that age stratification analysis, which is what is normally done, but has been hidden from us, then you find that the adverse events also cluster in these people that are aged, that have underlying conditions. And that sounds like, from what I’m learning from you, is that this excess mortality signal that you’re detecting that correlates with the inoculation campaigns may be stratified also by age. And that would be entirely consistent with all the other data.
Dr. Theo Schetters: Which is true. So if I break it up in three age groups, then you see that the most of the mortality is in the plus 80.
Dr. Robert Malone: Which is unfortunate because they’re the ones that need it the most.
Dr. Theo Schetters: Exactly.
Dr. Robert Malone: But we cannot look away from the truth,
Dr. Theo Schetters: But, Robert, at this point of time, do they still need vaccination? Because we talk about Omicron, we talk about a good level of herd immunity here. And so what is the risk now for the people of those ages?
Dr. Robert Malone: Which is why (among so among other things that I represent) I stand as the President of the International Association of Physicians and Medical Scientists. So we’re 17,000 that are only physicians and medical scientists, all verified, no nurses, not because we don’t like nurses, but it has to do with the positioning with the press and messaging. So that’s the basis for our organization.
Months ago, we came out with a press conference in a clear unequivocal statement that one can find at www.globalcovidsummit.org, where we made a clear, unambiguous statement. In our opinion, as an organization, these vaccines should be withdrawn. They are no longer justified on a risk-benefit ratio. And as the person who is responsible for the genesis of this technology, I’m often criticized. Didn’t I realize what I was doing? And there’s no way for me to have known that the normal standards for regulatory development and testing and clinical would be circumvented.
But I stand as someone who has intimate, detailed knowledge of the technology and its risks and benefits, the nature of the formulations, the role of the pseudouridine, all of those things.
It’s my opinion and that of the organization that I represent, that the data are now sufficiently clear that, in our opinion, the ongoing campaign for vaccination is no longer warranted.
Dr. Theo Schetters: I agree.
Dr. Robert Malone: And furthermore, it’s our opinion that early (multi-drug) treatment saves lives. That we now have a broad spectrum of early treatment options. All of the press attacks about ivermectin or hydroxychloroquine. Even if you set all those aside, there are plenty of other agents. The novel agents, monoclonal antibodies. Many things. What matters is that these… our elders, our high-risk individuals have immediate access to therapeutics.
Dr. Theo Schetters: Exactly.
Dr. Robert Malone: If they develop symptoms. Just like the President. Just like Tony Fauci. The same standard should apply to any of our high-risk individuals. But likewise, we should not continue with this ‘everything deserves the same hammer’.
Marlies Dekkers: One size fits all.
Dr. Robert Malone: Such as Paxlovid, with which a recent Science magazine op-ed clearly outlines that this protease inhibitor strategy against the main protease, which is the mechanism of Paxlovid, is highly susceptible to viral evolutionary escape.
Dr. Theo Schetters: Drug escape.
Dr. Robert Malone: And we are observing that. And it was a known risk with protease inhibitors. It is a known risk with HIV protease inhibitors. We know we know all of this science. I sat on the committee at NIH, the Foundation for the NIH called the ACTIV Committee, during the time when these drugs were being tested, the ACTIV trials. And it was explicitly acknowledged at that time that this single agent strategy was a total setup for evolutionary escape of the virus. You know this as a virologist. And what that means is not that we should not use the drugs as single agents.
Dr. Theo Schetters: No, but in combination.
Dr. Robert Malone: We should use them in combination and we should use them selectively for the people that need the most. And we have Pfizer, the manufacturer, who halted their clinical trials for Paxlovid in the normal risk individuals because it wasn’t working. It was not effective in people of average risk. Okay? So we have multiple lines of evidence that one should not just blindly use this drug every time somebody gets infected, we need to use these things wisely.
Dr. Theo Schetters: Yes. Like you have to do with vaccines.
Dr. Robert Malone: Just so.
Marlies Dekkers: Okay. Thank you both enormously. I think it was a very learning conversation for me. It was. And thank you for your time and thank you for coming to the Netherlands.
Dr. Robert Malone: My pleasure, and thank you for the opportunity to be here and learn from all of you. And I am so grateful to learn of your courage and your work. I certainly empathize with the academic backlash and the corporate media backlash and the censorship and propaganda and defamation and gas lighting that so many of us have experienced, but in the face of all that you continue to be courageous. And I thank you for that. I honor you.
@Edgar
The article does specify mRNA vaccines as you note, but the DNA vaccines are also associated with significant vaccine injuries, albeit they will have their own ratios of occurrence, yet I am unaware of what those ratios are.
Given you are about to take the second shot on the Novavax, I thought I might share what I have been able to ascertain on the latest reports that I have seen. Novavax is not very well represented in countries where they have pharmaco-surveilance data being collected. The largest report, I believe is from Eurovigilance out of Europe, where they have administered only ~216,000 shots and experienced about 2K adverse reactions – mind you this is all adverse reactions, both mild and severe.
Based on the data collected in Eurovigilance, Novavax has been labeled with warnings for anaphylaxis (shock), as well as paraesthesia (tingling sensation in the skin) and hypoaesthia (numbness usually in the skin). They have also collected reports of 5 cases of myocarditis/pericarditis, but they have yet to label any warning associated with myocardits/pericarditis with the Novavax shots. As a point of comparison, by this time in 2021, Pfizer was already labeled for myocarditis and thousands of cases had been reported, just in the US, but this was coincident with hundreds of millions of doses being administered as well. Additionally, as Dr. Malone notes in the article above, it has been accepted by some that the rate of occurrence of myocarditis with the mRNA shots is about 1 in 5,000, which is catastrophically alarming, but this is based on more than the pharmaco-vigilance data which is all that I have been able to locate for Novavax.
In Canada and Korea and elsewhere where I believe Novavax is employed more broadly, there is no useful pharmaco-surveilance tool collecting data in a useful manner, which is regretful. Additionally, the WHO has a pharmaco-vigilance tool called VigiAccess which collects data from all over the world, but it reports all reports for all Covid shots under each of the different vaccines, ie both Pfizer’s Cominarty and Novavax’s Covax products each have the same 4,134,959 cases listed, making VigiAccess the most useless mish-mash of spliced data possible.
In the US, I believe Novavax has only been being used for a little over a month, and they have no reports pulling up in OpenVAERS currently under the Novavax shot.
As you noted, there is very little spike and lipidnanoparticle present in the Novavax product, and it is a more traditional adjuvant based vaccine, so no spike factories are created in the body. The consequence of this is that the limited amount of spike that is injected in the shot is all the spike that the body has to deal with, and, consequently, it had been expected that this vaccine would likely provide fewer adverse events.
Regarding your delay in receiving the second dose, it is believed that the tight window between the first and second shots in the mRNA and DNA vaccines is associated with elevated number and severity of adverse events. It had been proposed that the period between the initial two shots might be spaced out more distantly, months as opposed to weeks, to reduce the number of such adverse events from occurring, which was ignored of course.
In any event, hope you find some relevance in all of this as you are about to take another shot. Be well.
@Ted
Is that due to Covid or the vaccine?
It’s a fair question to consider.
Dr. David notes says “New disability certificates issued per year” and it goes back to 2017. Consequently, in 2017-19 it would not include the virus or the vaccine as causes, in 2020 it would include the virus and other causes but not the vaccine, and in 2021 it would include either the vaccine or the virus as well as any other cause. It is noteworthy that the increase from 2019 to 2020 was actually less than the increase from 2018 to 2019, and then there was a seismic increase during 2021, with the implication that the increase occurred alongside the administration of 3-4 doses of the vaccine over the year of 2021. Does this indicate that the increase in disabilities were caused by the vaccine and not the virus? No, not necessarily. But if it was caused by the virus rather than the vaccine, why was there no significant rise during 2020, when the rate of increase was actually decreased (being careful here to indicate that the rate of the increase disabilities dropped, not the actual number of disabilities)? Lets restate this with actual values**. In 2018 there was an increase of 17.6% over 2017. In 2019, there was an increase of 18.7% over 2018. In 2020, there was an increase of 3.4% over 2019. In 2021, there was a 122% increase over 2020. So in 2020, the rate of increase was reduced as compared to the rate of increase in 2019, while the rate of increase of 2021 was shockingly elevated over the increase 2018, 2019, and 2020, based on the data provided in Dr. David’s tweet. It might be helpful to have a longer look back than just to 2017 but based on what we are looking at, there does appear to be a clear safety signal present in the data in 2021 that bears investigation.
Given the significant number of disabling cases associated with the vaccines (including neurological, cardiovascular and inflammatory symptoms among others) as recorded in VAERS and other pharmaco-surveillance databases and the Pfizer data, this sharp increase in disability certificates should draw significant attention to the possibility of the increase being caused by the vaccine rollout, particularly since there was nearly no increase in 2020. As with excess death rate, it would be useful to establish a prolonged baseline of 5-10yrs prior to 2020/2021 for comparison. Then this could be used to gain a better insight than the few years data offered in David’s tweet.
Honestly, perhaps there is some rational explanation for all of this which might indicate that the cause of the marked rise in disability certificates being issued in 2021 was actually related to the virus or something other than the vaccine. Right now, without any other explanation or information, I would argue that Occam’s razor suggests the vaccine is the most likely cause, IMHO, of course. Dissenting opinions or corrections, welcome, of course.
**Using the formula for the % rise from year 1 to year 2 :
[[(# in year2) – (# in year1)/(# in year 1) ] x 100%
@TED_
According to the article it looks like the mRNA Vaccines.
May I assume that this applies only to the mRNA vaccines. I have taken the first dose of Novavax, which is a protein based vaccine using traditional technology. It has an exceedingly favourable rating, with negligible or no side effects. Some 3 million doses were recently introduced into the US, with more on order.
Although delayed, I expect to get the second dose next week.
I think the PTB know everything, they are just killing off the “undesirables”, especially the elderly.
So 2021 was found to have more than double the number of “disability certificates” than were issued in 2020, and there are already far more such certificates issued in 2022 than in 2020 as well.
EDITOR
Ted Belman
tbelman3- at- gmail.com
Co-Editor
Peloni
peloni1986@yahoo.com
Customized SEARCH
ISRAPUNDIT DAILY DIGEST
Subscribe for Free
SUPPORT ISRAPUNDIT
If you are paying by credit card, when filling out the form, make sure you show the country at the top of the form as the country in which you live.



@Edgar
The article does specify mRNA vaccines as you note, but the DNA vaccines are also associated with significant vaccine injuries, albeit they will have their own ratios of occurrence, yet I am unaware of what those ratios are.
Given you are about to take the second shot on the Novavax, I thought I might share what I have been able to ascertain on the latest reports that I have seen. Novavax is not very well represented in countries where they have pharmaco-surveilance data being collected. The largest report, I believe is from Eurovigilance out of Europe, where they have administered only ~216,000 shots and experienced about 2K adverse reactions – mind you this is all adverse reactions, both mild and severe.
Based on the data collected in Eurovigilance, Novavax has been labeled with warnings for anaphylaxis (shock), as well as paraesthesia (tingling sensation in the skin) and hypoaesthia (numbness usually in the skin). They have also collected reports of 5 cases of myocarditis/pericarditis, but they have yet to label any warning associated with myocardits/pericarditis with the Novavax shots. As a point of comparison, by this time in 2021, Pfizer was already labeled for myocarditis and thousands of cases had been reported, just in the US, but this was coincident with hundreds of millions of doses being administered as well. Additionally, as Dr. Malone notes in the article above, it has been accepted by some that the rate of occurrence of myocarditis with the mRNA shots is about 1 in 5,000, which is catastrophically alarming, but this is based on more than the pharmaco-vigilance data which is all that I have been able to locate for Novavax.
In Canada and Korea and elsewhere where I believe Novavax is employed more broadly, there is no useful pharmaco-surveilance tool collecting data in a useful manner, which is regretful. Additionally, the WHO has a pharmaco-vigilance tool called VigiAccess which collects data from all over the world, but it reports all reports for all Covid shots under each of the different vaccines, ie both Pfizer’s Cominarty and Novavax’s Covax products each have the same 4,134,959 cases listed, making VigiAccess the most useless mish-mash of spliced data possible.
In the US, I believe Novavax has only been being used for a little over a month, and they have no reports pulling up in OpenVAERS currently under the Novavax shot.
As you noted, there is very little spike and lipidnanoparticle present in the Novavax product, and it is a more traditional adjuvant based vaccine, so no spike factories are created in the body. The consequence of this is that the limited amount of spike that is injected in the shot is all the spike that the body has to deal with, and, consequently, it had been expected that this vaccine would likely provide fewer adverse events.
Regarding your delay in receiving the second dose, it is believed that the tight window between the first and second shots in the mRNA and DNA vaccines is associated with elevated number and severity of adverse events. It had been proposed that the period between the initial two shots might be spaced out more distantly, months as opposed to weeks, to reduce the number of such adverse events from occurring, which was ignored of course.
In any event, hope you find some relevance in all of this as you are about to take another shot. Be well.
@Ted
It’s a fair question to consider.
Dr. David notes says “New disability certificates issued per year” and it goes back to 2017. Consequently, in 2017-19 it would not include the virus or the vaccine as causes, in 2020 it would include the virus and other causes but not the vaccine, and in 2021 it would include either the vaccine or the virus as well as any other cause. It is noteworthy that the increase from 2019 to 2020 was actually less than the increase from 2018 to 2019, and then there was a seismic increase during 2021, with the implication that the increase occurred alongside the administration of 3-4 doses of the vaccine over the year of 2021. Does this indicate that the increase in disabilities were caused by the vaccine and not the virus? No, not necessarily. But if it was caused by the virus rather than the vaccine, why was there no significant rise during 2020, when the rate of increase was actually decreased (being careful here to indicate that the rate of the increase disabilities dropped, not the actual number of disabilities)? Lets restate this with actual values**. In 2018 there was an increase of 17.6% over 2017. In 2019, there was an increase of 18.7% over 2018. In 2020, there was an increase of 3.4% over 2019. In 2021, there was a 122% increase over 2020. So in 2020, the rate of increase was reduced as compared to the rate of increase in 2019, while the rate of increase of 2021 was shockingly elevated over the increase 2018, 2019, and 2020, based on the data provided in Dr. David’s tweet. It might be helpful to have a longer look back than just to 2017 but based on what we are looking at, there does appear to be a clear safety signal present in the data in 2021 that bears investigation.
Given the significant number of disabling cases associated with the vaccines (including neurological, cardiovascular and inflammatory symptoms among others) as recorded in VAERS and other pharmaco-surveillance databases and the Pfizer data, this sharp increase in disability certificates should draw significant attention to the possibility of the increase being caused by the vaccine rollout, particularly since there was nearly no increase in 2020. As with excess death rate, it would be useful to establish a prolonged baseline of 5-10yrs prior to 2020/2021 for comparison. Then this could be used to gain a better insight than the few years data offered in David’s tweet.
Honestly, perhaps there is some rational explanation for all of this which might indicate that the cause of the marked rise in disability certificates being issued in 2021 was actually related to the virus or something other than the vaccine. Right now, without any other explanation or information, I would argue that Occam’s razor suggests the vaccine is the most likely cause, IMHO, of course. Dissenting opinions or corrections, welcome, of course.
**Using the formula for the % rise from year 1 to year 2 :
[[(# in year2) – (# in year1)/(# in year 1) ] x 100%
@TED_
According to the article it looks like the mRNA Vaccines.
May I assume that this applies only to the mRNA vaccines. I have taken the first dose of Novavax, which is a protein based vaccine using traditional technology. It has an exceedingly favourable rating, with negligible or no side effects. Some 3 million doses were recently introduced into the US, with more on order.
Although delayed, I expect to get the second dose next week.
I think the PTB know everything, they are just killing off the “undesirables”, especially the elderly.
Is that due to Covid or the vaccine?
From Dr. Eli David:
https://twitter.com/drelidavid/status/1557104807114162177
Accompanying graph shows:
2017: 22,296
2018: 26,213
2019: 31,105
2020: 32,165
2021: 71,258
2022*: 50,476
So 2021 was found to have more than double the number of “disability certificates” than were issued in 2020, and there are already far more such certificates issued in 2022 than in 2020 as well.