
There is not evidentiary correlation between cases and vaccination rates
By Justin Hart, REVOLVER NEWS
I have no idea how this paper made it past the censors but there it is! This was published a month ago but didn’t receive much fanfare and now we know why—it confirms what we’ve been saying for months now: the vaccines have not stopped and likely will not stop the pandemic.
Back in July we tweeted that the CDC data mapping vax rates to COVID-19 case rates shows ZERO impact of the former on the latter:
 <
<
>
 <
<
>
<
>
 <
<
>
 <
<
>
<
>
<
>
July 26th 2021
<
>
<
>
We’ve written in these pages multiple times about the same phenomenon. Yesterday, Dr. Jay Bhattacharya of Stanford tweeted:
“There is a lot to learn from this graph, but most obviously, the COVID vax does not stop infection. The vax provides a private benefit (protection vs. severe disease), but limited public benefit (protection vs. disease spread). So what is the argument for mandates?”
Now this Harvard research notes:
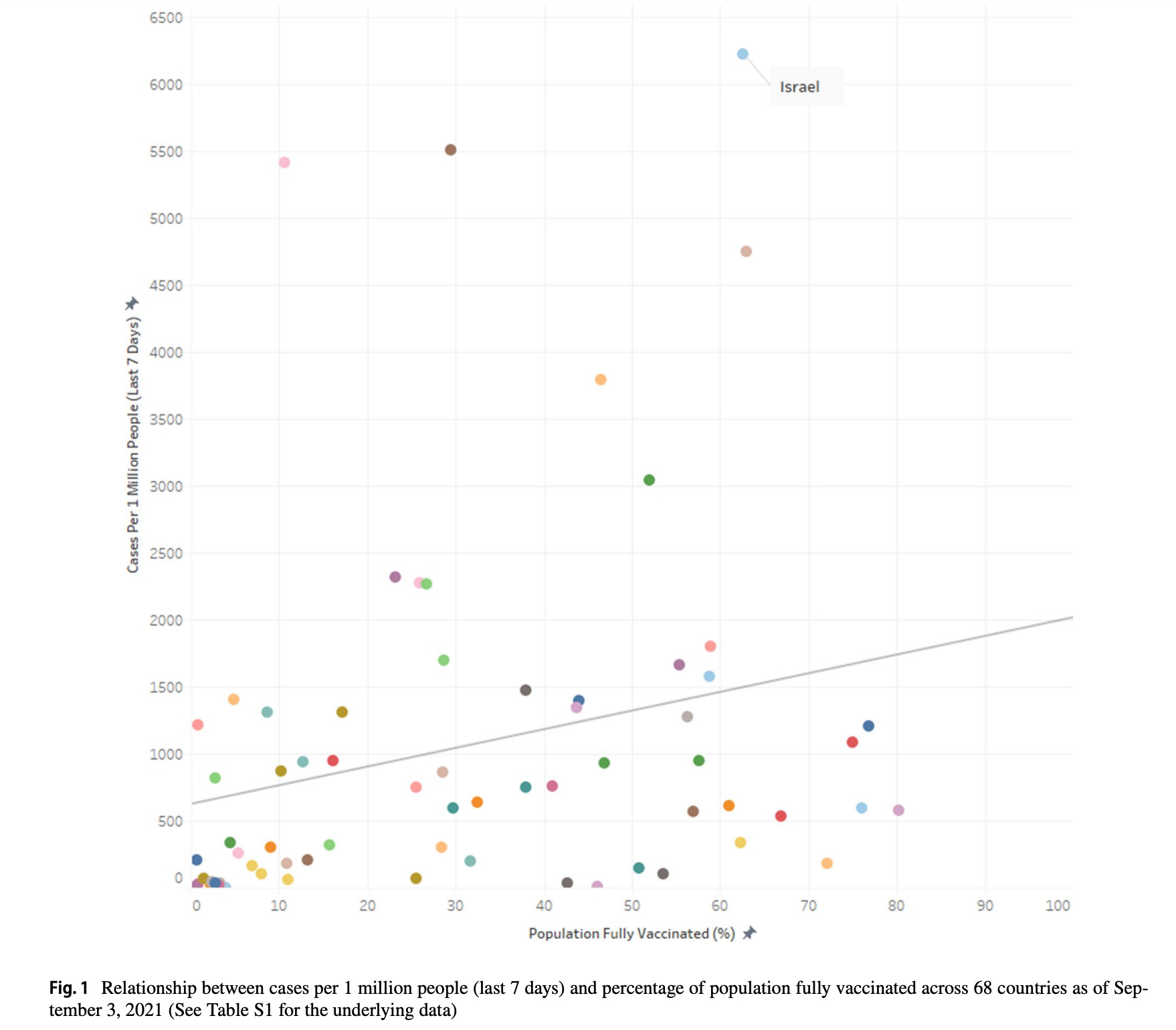
At the country-level, there appears to be no discernable relationship between percentage of population fully vaccinated and new COVID-19 cases in the last 7 days (Fig. 1). In fact, the trend line suggests a marginally positive association such that countries with higher percentage of population fully vaccinated have higher COVID-19 cases per 1 million people.
<
>
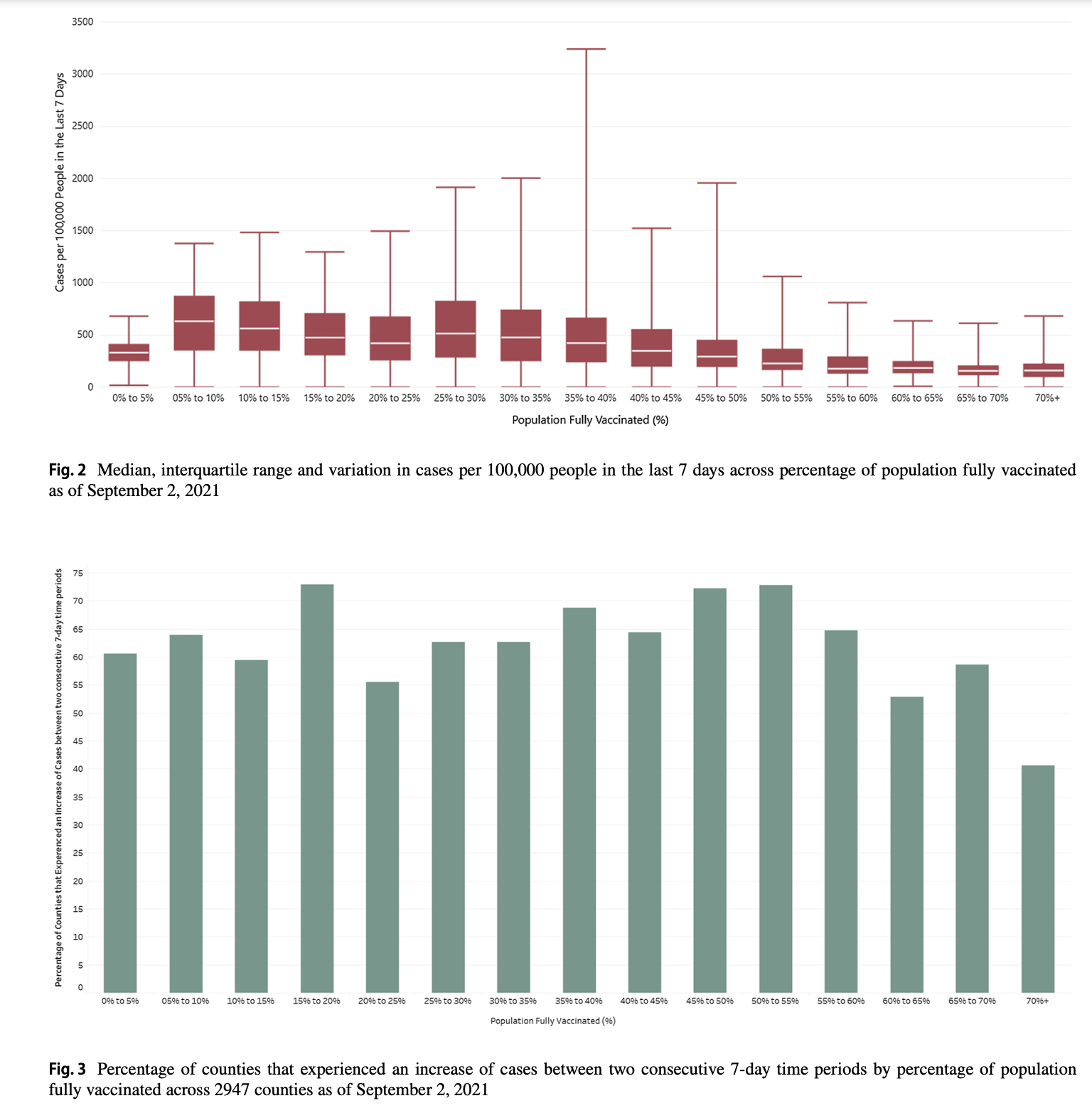
When they got down to the U.S. county level the relation was even less discernible:
<
>
They conclude:
The sole reliance on vaccination as a primary strategy to mitigate COVID-19 and its adverse consequences needs to be re-examined, especially considering the Delta (B.1.617.2) variant and the likelihood of future variants
Feel some vindication folks. We were right.


@Adam
I and Hart labeled the study as a Harvard study because the lead author is on the Harvard staff and the funding likely came from the Harvard T.H. Chan School of Public Health.
If you open the link to open the webpage with the study and tap on the authors’ names it will give you their credentials. Under the lead author, Subramarian, it states
Here is some background on the Harvard School of Public Health being renamed as it is today:
https://www.hsph.harvard.edu/magazine/magazine_article/the-story-of-t-h-chan/
Kumar is likely the one who performed much of the leg work, but with two authors, perhaps not. He is from Turner Fenton Secondary School, Brampton, ON, Canada.
I really know not the first thing about either author beyond their names and collegiate affiliations.
You will likely never hear me offer praise or ridicule for someone when I have no certain knowledge of their background such as the author’s here. They are part of the faculty of the Harvard School of Public Health, that should qualify them well enough to whatever such things might impress or dissuade you of their import. I find such details useful, but I hold no such intimate knowledge of most of the authors of the hundreds of studies that I have read over the past many months. Occasionally, I will be aware of the author’s background, such as was the case with Dr. Lawrie, and I offer such details as they are relevant, but I have no info to share regarding Subramarian or Kumar. As part of the Harvard staff, it is unlikely they have a reason to place the vaccine in a poor light, and the fact that they titled the study as showing no effect when there was in fact a definite effect should qualify something about either their intent or what was needed to get their work published.
I discussed this study elsewhere on Israpundit a few days before Ted posted it here, though I am not certain under which article. As I noted then and below, a retrospective study is useful but rarely conclusive, even though such parameters have been employed to declare pregnant women being safe for vaccination and myocarditis as being less than what some prospective studies have shown. Such low standards to ‘prove’ a lack or limit of safety concern are very worrisome as it is a insupportable level of evidence to base a firm conclusion of certain safety upon. But safety concerns found in a retrospective study are always significant, as oppose to a lack of safety concerns. The two standards can not be assumed to be interchangeably valued. Vaccines now and in the past have always been held to the standard of proving a level of safety, rather than assuming it. There was also never a sense of a little death is acceptable, much less thousands. This is why in years prior to 2021 there have never been any great number of deaths listed in VAERS. Until Covid, that is. Now retrospective studies are used to prove safety concerns unwarranted and tens of thousands of deaths in VAERS and other pharmaco-surveillance mechanisms are ignored entirely.
Also the Journal of Epidemiology is a well reputed journal, for whatever that means in 2021.
If you can be specific about anything you feel I was confusing or misleading, let me know and I would be happy to clarify or correct my comments.
@peloni. Peloni, a correction to my last post. The article in the European Journal of Epidemiology does not contain any reference to the author’s having any connection with Harvard University. In fact it says nothing whatever about the professional credentials. I therefore have no idea why Mr. Hart and you refer to this as “the Harvard Study.”
I apologize for posting that you had not posted a link to the Springer article. This is not correct. When I searched through the fairly long number of comments posted about this article, I found your reply to my initial question asking for a link.
I also found the link in in Mr. Hart’s article. I missed it because he didn’t provide a URL, but rather red words which when pressed linked one directly to the page. But I suffer from from red-green color blindness, which is why I missed the link.
At the time I made this post I was focused on your most recent post about the “Harvard study.” I did not look through all 24 of the previous posts, many of them from you. This was one reason for my confusion.
But I still find some terms of reference in your comments as well as those of Mr. Hart that seem to me to be confusing and even misleading, although of course not internally. You both refer repeatedly to the “Harvard Study.” But when I opened your link to the study and read it, I found no indication that the medical journal that published it was published by Harvard University or even connected with that university. Perhaps I missed something about that. If so, please enlighten me.
I did find a reference to one of the author’s having a connection to Harvard in the brief introduction to the article. But I didn’t find any statement that the second author was Harvard-Affiliated.
It still would have helped me if you had given more basic bibliographic information about the article in the text of your comments itself. Also, if Mr. Hart had done that. That would have reassured me that we were discussing a genuine article in a medical journal written by genuine scientists. I always find these things easier and quicker to learn when they are spelled out in the text of an article or comment, rather than just referenced in a link.
You also might have discussed the authors and their scientific credentials, and why you regard them as experts in this particular subject.
I have to go now. More later.
@Adam
I am really uncertain why what I wrote confused you. You questioned where the link and date and authors were for the article Ted posted by Justin Hart, or that was my understanding of your comments and perhaps I misconstrued your meaning as your own comment was a bit vague as to what . I offered you the authors name and date and a direct link to download the article. The title for the article is “Increases in COVID?19 are unrelated to levels of vaccination across 68 countries and 2947 counties in the United States” and it can be found in the Journal of Epidemiolog, but if you use the link I placed in the post, it will download the article directly for you.
In the article that Ted posted by Hart, there are also at least 2 links in his comments for the study by Subramanian. There is a link in the first line of his comments above:
under the hyperlink found in “this paper”, and he again links it half-way down when he states:
under the hyperlink found in “this Harvard research”. I am not sure if the link is not working for you, but I will share it again here:
https://link.springer.com/content/pdf/10.1007/s10654-021-00808-7.pdf
It is a downloadable PDF that you have to open once it is downloaded.
Altrernatively, here is a direct online link, perhaps that would be more convenient for you to use:
https://doi.org/10.1007/s10654-021-00808-7
If this is not the article to which you are referring, let me know and I will try to get you the info you are looking for or offer what clarity I can to whichever comments of mine that have left you uncertain of my meaning.
I have received some important “anecdotal evidence” of the shortcomings of the vaccine from my Chabad rabbi. His father, a man of 79 years, completed a course of vaccination in June of this year. But just in the past two weeks, he felt very ill, tested positive for Covid-19 and was hospitalized. I think it was a hospital in Queens. My rabbi was very worried about his father, as was clear when he spoke about the matter to our congregation. He says his father is out of the hospital now, and feeling better.
I think we can call this a “breakthrough case” after only four months after he was vaccinated.
My rabbi also said his father was treated with an “infusion” of “antibodies” and responded well to this treatment. The rabbi knows no more about medicine than I do (well, a little bit more), so I don’t know what was included in this “infusion.” But I assume that it included monoclonal antibodies.
Dr. Thomas Siler’s article in American Thinker is the best, succinct and clearly written summary of the “anti-vaxxer’s” (or more accurately pro-choicer’s) case that I have seen. Ted, I hope you will publish it in full hear, with permission from AT of course.
@peloni. Peloni, I feel uncomfortable writing this to you in view of how you have kept us informed about Covid19 and other medical matters over the past several months. But I remain concerned about your non-mastery of English written prose. I don’t know anything about medicine, but I taught English composition for many years to undergrads.
In your post just above this one, you appear to be talking about two different studies at once, without distinguishing between the two.
Neither the author of this article nor yourself in your comments about it provide the necessary bibliographic information about the study (where, when by whom published, authors). The rest of us thereby cannot find the study, read it and judge the author’s conclusions for ourselves.
I wish I could could give you a tutorial in prose composition so that you could remove these bugs in your writing style and and communicate all of your vast knowledge more clearly to the medically uninitiated. But I don’t know how to do this over the internet, and I guess neither of us would have enough time to do for such a course of study.
Many thanks and all my best as always, Adam.
Here are the authors:
S. V. Subramanian · Akhil Kumar
It is dated from Aug17, 2021
Justin Hart linked to the study above, but here it is:
https://link.springer.com/content/pdf/10.1007/s10654-021-00808-7.pdf
@Adam
“The charts published by Ran Israeli are cut off so as not to show the data 2021, although you can see on the right hand edge of the screens that the charts do include entries for 2021. Suspicious. Source for the August 2021 data not given ”
The charts aren’t cut off in my browser. 2021 was the point of the chart.
He has 3800 non-Covid deaths, 2627 fully vaccinated, 15 partially vaccinated, and 222 unvaccinated.
The data is incomplete which makes his findings, compared to past years including 2020, even more alarming.
He does give the sourcing for his data:
https://twitter.com/RanIsraeli/status/1448754236657971204
and he noted this again when asked about it here:
https://twitter.com/RanIsraeli/status/1448981798365667331
The charts published by Ran Israeli are cut off so as not to show the data 2021, although you can see on the right hand edge of the screens that the charts do include entries for 2021. Suspicious. Source for the August 2021 data not given. Doesn’t prove, however, that it is incorrect.
An inadequately documented study.The author doesn’t identify his source or provide links to it. Which Harvard study? Published where and when? Authors?
Thank you, Peloni for your rebuttal of Bear et al:”Meanwhile, the vaccines have serious side effects. Also the first two weeks-post-vax provide a window in which the virus has an increased opportunity to infect vaccinated people. In spite of this or because of this, the vaccinated who become ill in that 2 week period are added to the unvaccinated column. You need have no medical knowledge to understand this is purposefully injecting a desired bias into the stats that you see as being very good. We know injecting the spike creates antibodies. We also know that it inhibits the immune system. By ignoring the consequences of the inhibited immune system, you have eliminated any critisism possible against the vaccines.”
This is PRECISELY the problem, with all aspects of this “pandemic”, namely, false science in the service of Fauci & Co, some of the richest people in Washington, who are making their fortunes through the manufacture and sale of not only the vaccines but of the virus itself.
Robert Kennedy Jr. produced a video a short while ago, describing the enormity of the Fauci Empire, and its tentacles throughout the medical community. Sorry, no link yet.
Avi Barak, the photographer who reported the FaceBook iMOH scandal has posted a video of
https://twitter.com/i/status/1449270332779548673
@Bear
Covid is easy to remedy and eliminate, it would seem. India has shown us this fact, and Japan(https://www.worldometers.info/coronavirus/country/japan/) is now well on its way with a similar outcome. In truth, this virus is very easy to kill if treatment is employed. Dr. Urso has over 30 drugs that he employs to treat the disease with ease, if treated early. There are also some very strong evidence showing the likelihood that medical prophylaxis could replace the vaccines with fewer breakthroughs and no side effects, but more testing is required, ie $$. Meanwhile, the vaccines have serious side effects. Also the first two weeks-post-vax provide a window in which the virus has an increased opportunity to infect vaccinated people. In spite of this or because of this, the vaccinated who become ill in that 2 week period are added to the unvaccinated column. You need have no medical knowledge to understand this is purposefully injecting a desired bias into the stats that you see as being very good. We know injecting the spike creates antibodies. We also know that it inhibits the immune system. By ignoring the consequences of the inhibited immune system, you have eliminated any critisism possible against the vaccines.
The issue of serious side effects in enormous numbers is always ignored when people speak of the value of the vaccines, as if those suffering thes side effects have no role in this ongoing drama. For example, 9,500 cases over 4months just in the US have reported myocarditis and there is still a backlog of untold numbers in addition to this, as confirmed by Dr. Rose, Dr. Malone, & Dr. McCullough. Myocarditis has a “mortality rate of 25% to 56% within 3 to 10 years”(https://www.ncbi.nlm.nih.gov/labs/pmc/articles/PMC3370379/). The reason myocarditis shows up in children so clearly is due to the fact that children don’t have heart ailments or disease issues that chest pain will be attributed to such as is the case in someone older. So someone 50yrs old with a heart problem won’t attribute chest pain to the vaccine. Someone 75yr old won’t attribute sudden death to the vaccine. Especially in this political climate. So the elderly are likely being affected as well as the young, but if we don’t look, we won’t find it. And if we don’t find it, we can’t remedy the harms that are resulting from this vaccine campaign.
Seems clear to me that the stats in Israel show vaccination has a super positive effect on keeping people alive, not getting very sick and also reduces greatly the likelihood of getting Covid-19. This may not be perfect and drugs to fight the disease certainly should be part of the battle against
Covid-19. Several promising drugs are about to be approved and some certainly should be repurposed.
October 16, 2021
The Unvaccinated Are Looking Smarter Every Week
By Thomas T. Siler, M.D.
— https://www.americanthinker.com/articles/2021/10/the_unvaccinated_are_looking_smarter_every_week.html
“…It has been shown now that the vaccinated equally catch and spread the virus. Vaccine side effect data continues to accumulate that make the risk of taking the vaccine prohibitive as the pandemic wanes. Oral and IV medications (flccc.net) that work early in the treatment of COVID-19 are much more attractive to take now as the vaccine risks are becoming known, especially because the vaccinated will need endless boosters every six months…”
The new VAERS report is now available. The myocarditis cases is now at 9470 cases. One week ago it was approximately 8600 cases. That is an increase of clinical reports of 800 new case reports in a week – for all of 2020 there were 44 cases as comparison. Each report requires approximately 30min. to complete if the system does not time out and force you to either abandon the task or start again. This is terribly concerning.
On a related note of the topic of myocarditis associated with vaccination, the study completed by Dr. Rose and Dr. McCullough on Myocarditis Adverse Events in the VAERS was subjected to “Temporary Removal” without contacting either author prior to this action to mediate or remedy any concerns or disputes.
Dr. Malone’s comment on this removal:
This is from Ran Israel who identifies himself as a Computational Biologist / Regulatory Affairs Specialist on twitter.
He is looking at all cause mortality for the month of Aug going back 10yrs. His findings are shocking. For 2010-2019 the all cause mortality was 3500 or less. In 2020 it was 4000. Thus far this year, it is nearly 4500, and of this 3800 is for non-Covid causes. Recall that 20% of 2021 is yet to come and all the numbers for the first 9.5months are not yet included in the column for 2021.
https://twitter.com/RanIsraeli/status/1448752684031479810/photo/1
I hope this is proven to be wrong
This is from Ran Israel who identifies himself as a Computational Biologist / Regulatory Affairs Specialist on twitter.
He is looking at all cause mortality for the month of Aug going back 10yrs. His findings are shocking. For 2010-2019 the all cause mortality was 3500 or less. In 2020 it was 4000. Thus far this year, it is nearly 4500, and of this 3800 is for non-Covid causes. Recall that 20% of 2021 is yet to come and all the numbers for the first 9.5months are not included in this chart for 2021.
https://twitter.com/RanIsraeli/status/1448752684031479810/photo/1
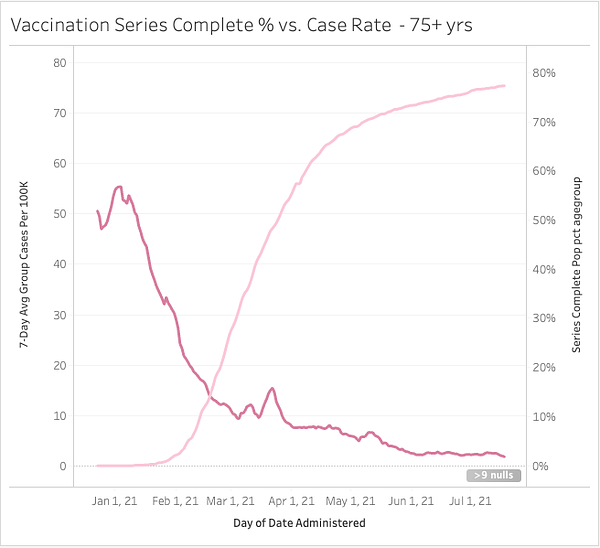
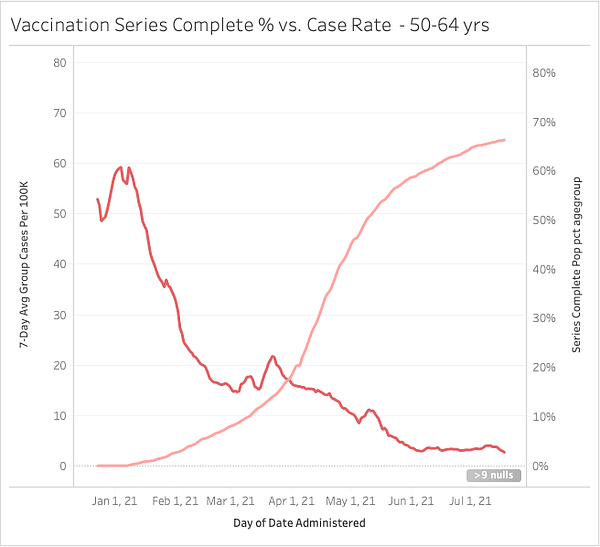
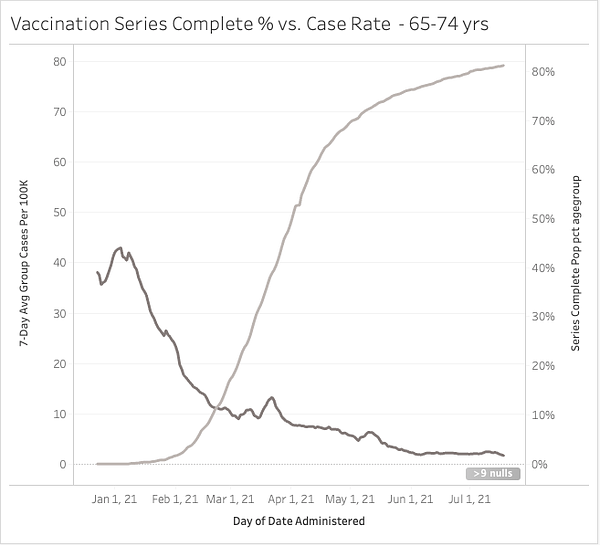
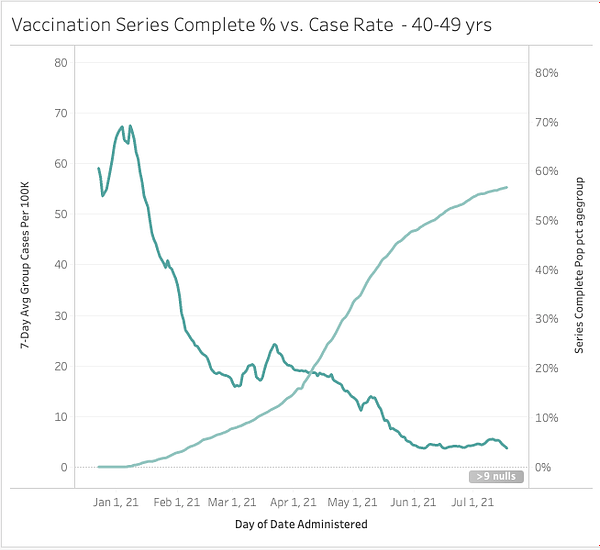
All of the charts of the percentage of “cases” for various age groups support the view that the vaccines are highly effective in reducing cases of Covid-19, at least for a time, even though the author of the article denies this.
However, Peloni is correct in pointing out that the way “cases” are defined and the way “vaccinated” and “unvaccinated” are defined has a built-in bias.. This is a valid point concerning the possible unreliability of these statistics.
I do think the preponderence of evidence indicates, without proving absolutely and beyond all reasonable doubt , that the vaccines are effective in preventing illness and death from cv19-2, at least for about six months.
However, this certainly does not mean that the over-all response to Covid-19 by the world’s political and medical establishments has been helpful or even honest. There is overwhelming evidence that some medications are highly effective in treating cv-2, and even in reducing the likelihood of becoming sick with it. Yet the world’s government heath departments have gone so far as to prohibit the use of some of these medications and taken steps to prevent doctors and patients from obtaining supplies of these medications. This has probably increased the death rate from cv19-2, both before and after the vaccines were introduced. This to my mind is the moral equivalent of mass murder. It is difficult to explain such behavior by government, medical and pharmaceutical establishments except by positing some form of corruption and conflicts of interest.
There are also legitimate questions about the safety of the vaccines, such as the possibility that they may increase the risk of patients developing many diseases other the Covid. While this has not been proved, some of the hypotheses formulated by competent physicians that this may happen, or even has already happened, are plausible. But the the infectious disease departments of the world’s governments have not even attempted to monitor the use of the vaccines to determine if they do in fact increase the risk of other diseases. Monitoring boards have not even been established for the vaccines, as used to be required by law at least in the United States.
It is as if the world’s government have saved people from dying of cv19-2 with one hand, while increasing the likelihood that they will die of cv19-2 , as well as many other diseases, with their left hand. Very sinister and troubling.
Only confirms my decision – indeed, my insistence! – to NOT be vaccinated with ANY of these experimental drugs, which seem to be impossible to separate from many instances of poison being injected into one’s body!!
@peloni
“you have to work with what you have”
You can’t make a silk purse out of a sow’s ear.
If you analyze crap, your conclusions will be crap.
It is impossible to account for all the biases and distortions.
The only way to do it, is to expand the Frontline Doctors and give them the authority to collect all the CLINICAL information but it is impossible anyway, it just cannot be done for many reasons.
@Raphael
Also the findings of this study were consistent when looking at just the least vaccinated couties and most vaccinated counties as follows:
Of the top 5 counties that have the highest percentage
of population fully vaccinated (99.9–84.3%), the US Centers for Disease Control and Prevention (CDC) identifies 4
of them as “High” Transmission counties.
@Raphael
Not really. If your data is crap, you still need answers. So, you have to work with what you have, knowing what you know, unless what you know doesn’t tell you anything, but I think it does. A level of certainty can be gained by considering relative biases. Your conclusion would be fairly stated if the data collection and manipulations were being done in an unknown pattern or without a certain and consistent bias. The unfortunate reality is that these manipulations have always had a certain and consistent bias – counting the vaccinated dead as unvaccinated, testing vaccinated subjects at much lower sensitivity than unvaccinated people, and testing the vaccinated more frequently than the vaccinated. The dead have been counted with the unvaccinated regardless of their vaccine status upto 2wks during which we know that 40-100% increases of vaccine failures can occur(https://cdn.substack.com/image/fetch/w_1456,c_limit,f_auto,q_auto:good,fl_progressive:steep/https%3A%2F%2Fbucketeer-e05bbc84-baa3-437e-9518-adb32be77984.s3.amazonaws.com%2Fpublic%2Fimages%2F3efbd37b-4957-4c1d-8357-f842d347808b_2627x1233.png). Also, the PCR test itself produces high numbers of false-positives in both the low-sensitivity used on vaccinated and in the higher-sensitivity used on the unvaccinated, but the false-positives are exponentially higher in the higher-sensitivity setting used with the unvaccinated. It is not an opinion that these actions would all routinely reduce the positive-rate among the vaccinated as well as reduce the death-rate among the vaccinated. Hence, there would be a significant bias advantaging, almost protecting, the vaccinated group from negative associations of increased cases or increased deaths when compared with the unvaccinated. This is called a survivor-ship bias, as all survivors are counted in and all who fail to survive are counted out.
No one could fairly give an estimate of the level of vaccine-casualties, ie an actual value – I think this is a fair statement. Still, the relative advantage in testing and counting deaths between the vaccinated and the unvaccinated is fairly obvious, I believe. By having the vaccinated tested less frequently, tested with fewer false positives and counted for two weeks as unvaccinated should they die, all provide a very strong relative bias favoring the vaccinated to the disadvantage of the the unvaccinated. This was no accident, I believe, but if it was, the accidents kept falling in a way to disadvantage the unvaccinated. The fact that this study above showed a positive association with disease among nations and counties with higher vaccination rates appears highly significant because it means that all the bias or selective advantages designed to protect the vaccinated population was not enough to show a consistent benefit to the vaccinated. Stated differently, the vaccinated had a built in buffer that should have shown a benefit for vaccination. The fact that this buffer was overcome is very worrisome.
If the study showed that the vaccine was beneficial, you could say the results were not necessarily balanced because of the built-in biases supporting the vaccines, and then you would have to tease out how the bias affected the outcome, which would never be possible.
We should look at a timeline of these charts, monthly or bi-monthly, and see if things are shown to be either more random or more consistent. It is very revealing that these biased factors to advantage the vaccines’ image did protect it with a positive benefit in any context or date, ie there should have been a great deal of bias to overcome. Hope this is clear.
how to prove those screaming YES to vax are vaxing?????
Eddie
That the “data” has been so badly manipulated, for so long, casts doubt on any numbers-based report, even for those of us who seek vindication. No?
This analysis was very alarming, especially the increased slope of the line on Fig. 1. It would be bad enough if the line was flat, ie no relationship, but the positive association between cases and vaccination is disturbing. I would like to see this series of charts completed in a monthly or bi-monthly basis from Dec to present to display the evidence of this association over time, ie when was the slope negative and when did it bottom out and begin to become positive.
It should be noted that they considered the lag in protection and so then considered the results of the same analysis with a 1 month lag post-injection and they still found no benefit for vaccination even with a 1-month lag post-injection. This evidence is VERY HARD to reconcile with forced mandates.
Israel’s 7-day average would still be above the line in that chart, while the actual number for yesterday would be barely below it. Though the slope of the line is likely altered, either higher or lower than seen in this chart.